
5 Documentation Errors Costing Emergency Departments Millions (AI Prevention Guide)
Emergency department documentation errors cost hospitals millions annually. Learn the 5 most expensive error types and how AI prevents revenue loss.

Most hospitals carefully track denial rates but miss the documentation errors that drive them. In emergency departments, documentation gaps are not just quality issues. They are revenue leaks that can cost the average ED between $500,000 and $2 million each year.
These are not coding errors or billing mistakes. They are gaps in clinical documentation that occur during patient care and later trigger denials, downcoding, and compliance exposure. This is not about physician competence. Emergency physicians manage multiple critically ill patients under intense time pressure. Documentation errors happen because of systemic workflow constraints, not individual failure.
This article identifies the five most expensive documentation error types, quantifies their financial impact, and explains how technology can prevent them before they cost money.
The Five Most Expensive Documentation Errors in Emergency Departments
These documentation gaps consistently appear in denied claims, payer audits, and revenue cycle reports across emergency departments nationwide.
1. Incomplete Medical Necessity Documentation
Medical necessity explains why a patient required emergency department evaluation rather than urgent care or a clinic visit. When charts do not make this clear, payers deny claims or downcode the visit.
This often happens because what is obvious in the moment does not get captured in the note. A physician evaluating a 55-year-old with chest pain knows why the ED is the right setting. But if the chart lists only “chest pain” without risk factors, symptom severity, time course, or other features that suggest an acute process, the encounter can read as clinic appropriate.
Cost per occurrence: $50 to $150 per denied or downcoded claim. If 10 percent of a 50,000 visit department has weak medical necessity documentation, that is roughly $375,000 in annual loss from this issue alone.
Real example: Chart documents “chest pain, normal EKG, troponin negative, discharged.” Payer denies payment stating the chart does not establish why ED evaluation was necessary. Missing elements include cardiac history, relevant risk factors, and symptom characteristics that warranted immediate evaluation.
Research proves that documentation deficiencies are a common driver of claim denials, and medical necessity gaps are a frequent issue in emergency department billing.
2. Missed Procedure Documentation
Emergency physicians perform dozens of procedures daily, including laceration repairs, joint reductions, incision and drainage, and foreign body removal. Each one represents billable revenue. When procedures are not documented with the required elements, that revenue is often lost.
This typically happens because physicians are prioritizing the most critical patients. A “simple” laceration repair can feel minor compared to the trauma next door. The repair gets done, it is explained to the patient, but the formal documentation, including indication, technique, complications, and time, never makes it into the chart.
Cost per occurrence: $100 to $400 per undocumented procedure. If each physician misses five procedures per month and you have 12 physicians, that is 720 missed procedures annually. At an average value of $200 each, that is $144,000 in lost revenue for care that was delivered.
Real example: A physician reduces a dislocated shoulder, discusses post-reduction care, and discharges the patient. The chart mentions “pain management provided” but contains no formal procedure documentation. The coder cannot bill for the reduction. Revenue lost: $300 to $400.
3. Undocumented Critical Care Time
Critical care billing offers significant additional reimbursement for time spent managing critically ill patients. It requires specific documentation, including total time spent, clear indication the patient met critical care criteria, and justification for the intensity of physician involvement.
This often happens in the chaos of resuscitation. Multiple providers manage a crashing patient. The emergency physician spends 45 minutes at the bedside directing care, but documentation happens later when details are less clear. Start and stop times are not captured. The complexity that justified critical care attention is not explicitly stated.
Cost per occurrence: $200 to $400 per missed critical care claim. If physicians miss two to three appropriate cases per month across 12 physicians, that is 360 missed opportunities annually. At $300 in average additional revenue, you are losing $108,000 for work already performed.
Real example: A septic patient requires continuous monitoring, multiple interventions, and 50 minutes coordinating care. The chart documents the clinical course but does not specify time or explicitly state that critical care criteria were met. The visit is billed as a level 5 E and M instead of critical care. Revenue lost: $350.
4. Insufficient Medical Decision Making for Billed Level
Emergency department E & M billing levels depend on medical decision making complexity. Level 4 and level 5 visits require documentation that shows differential diagnosis breadth, data reviewed, and patient risk. When charts do not clearly document this thinking, payers downcode.
This happens because clinical reasoning does not automatically translate into documentation. A physician managing a complex, multi system presentation is weighing diagnoses, risk stratification, and management decisions in real time. But if the chart only includes the final diagnosis and treatment plan, without showing the reasoning, the documented complexity does not match the care delivered.
Cost per occurrence: $30 to $80 per downcoded claim. If 15 to 20 percent of level 4 and level 5 charts have insufficient medical decision making documentation, and you bill 20,000 higher level visits annually, that is 3,000 to 4,000 vulnerable charts. At $50 average loss, you are losing $150,000 to $200,000 annually.
Real example: A complex abdominal pain patient. The physician considers appendicitis, ectopic pregnancy, ovarian torsion, kidney stone, and bowel obstruction. Labs, imaging, and a specialty consultation are ordered. The chart documents “abdominal pain, CT negative, discharged with pain management.” The differential, risk assessment, and data interpretation are not documented. The payer downcodes the visit from level 5 to level 4. Revenue lost: $60.
Studies on E & M documentation suggest that insufficient medical decision making is a common driver of downcoding, particularly in emergency medicine where clinical complexity often exceeds what is captured in the chart.
5. Missing Billing Critical Elements
Every emergency department chart needs baseline elements for billing, including a complete history of present illness, review of systems, physical exam, and clear medical decision making. When these are incomplete, charts cannot support the billed level and often require time consuming queries.
This happens because of interruptions and multi patient management. A physician starts documenting the history, gets pulled into a trauma, then returns later and cannot remember what was already captured. The review of systems may be partially completed. Exam findings may cover one system but omit others. Orders may be placed without clearly documenting the indication.
Cost per occurrence: $20 to $60 per incomplete chart that requires queries, plus reimbursement delay. If 20 percent of charts need queries because of missing elements across 50,000 annual visits, that is 10,000 queries. If each query takes 15 minutes of combined HIM and physician time valued at $100 per hour, that is $25,000 in wasted labor annually, plus delayed cash flow on those claims.
Real example: The chart documents abdominal pain. A CT is ordered and completed. The chart closes with “CT negative, discharged.” There is no documented indication for why the CT was ordered, no interpretation, and no differential diagnosis to support the imaging decision. The coder must query the physician before submitting the claim. The claim is delayed by three weeks.
True Financial Impact
Documentation error costs extend beyond the immediate denied claim.
Direct Costs:
Denied claims represent revenue you may never recover. Many emergency departments do not have the resources to appeal every documentation related denial, so the revenue often disappears.
Downcoded claims mean payment at a lower service level than the care provided. A level 5 visit downcoded to level 4 can cost $50 to $80 per occurrence. Over thousands of visits, this adds up quickly.
Undocumented care is pure revenue leakage. The service was delivered and the patient benefited, but without complete documentation, it cannot be billed.
Indirect Costs:
Audit exposure increases when documentation shows consistent gaps. Payers notice trends, and patterns can trigger more intensive audits with repayment demands and compliance penalties that exceed individual claim amounts.
Query burden creates operational inefficiency. HIM staff spend time tracking down physicians for clarifications, and physicians spend time responding to queries about patients seen weeks earlier. This delays claim submission and impacts cash flow.
Compliance penalties can dwarf individual denials. When audits reveal systematic issues, payers may seek repayment across lookback periods and impose additional penalties. A pattern affecting 10 percent of charts can create seven figure exposure.
Cumulative Effect:
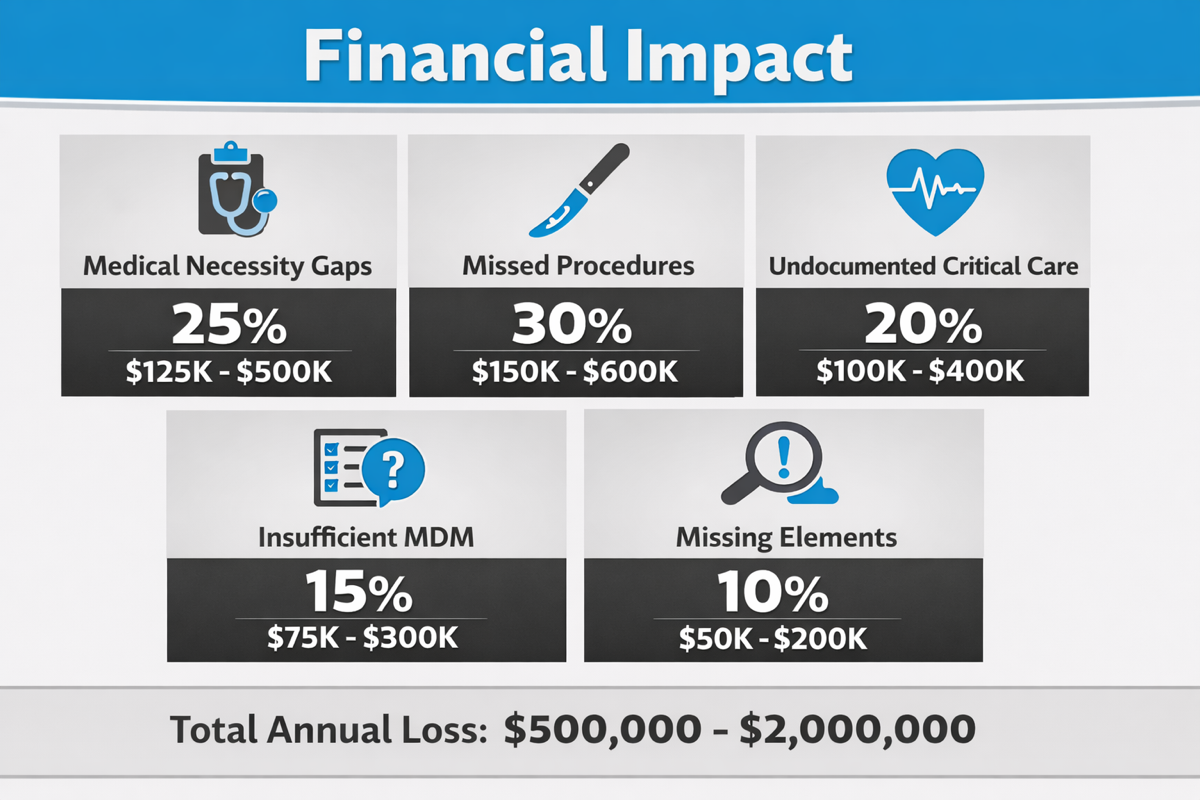
A typical 50,000 visit emergency department making these five errors can lose $500,000 to $2 million annually. A rough breakdown by error type:
- Medical necessity gaps: 25% ($125,000 to $500,000)
- Missed procedures: 30% ($150,000 to $600,000)
- Undocumented critical care: 20% ($100,000 to $400,000)
- Insufficient MDM: 15% ($75,000 to $300,000)
- Missing elements: 10% ($50,000 to $200,000)
Technology that catches documentation gaps in real time typically costs $100,000 to $200,000 annually for mid size emergency departments. If it prevents even 40 percent of errors, the return on investment can be immediate.
Why These Errors Happen in Emergency Departments
Documentation errors are not about physician competence. They are the predictable result of trying to produce complete documentation inside an emergency department workflow.
Workflow Pressure
Emergency physicians manage three to four patients at different stages at the same time. One may need immediate resuscitation. Another is waiting on a consult. A third has imaging results that need interpretation. A fourth is ready for discharge. Documentation competes with direct patient care, and when a trauma activates, charting often stops.
Time Constraints
Patient volume creates relentless pressure. The next patient is waiting and the waiting room is full. Spending 15 minutes on comprehensive documentation can mean another patient waits longer. Many physicians finish charts after the shift ends, reconstructing details from hours earlier when memory has faded.
Multi-Patient Context Switching
Managing multiple patients at once makes it easy to lose details. Which patient had cardiac risk factors. Which chest pain patient had a troponin drawn. Which encounter met critical care criteria. What starts as “I will document that in a minute” becomes “I cannot remember which patient” a few hours later.
EHR Design Gaps
Many EHR systems are not designed around emergency department workflows. Templates often do not prompt for billing critical elements at the right moment. It is easy to close a chart without realizing required fields were skipped. The gap is often discovered only when HIM reviews the chart for coding.
Complexity of EM Billing Rules
Emergency medicine billing rules are complex and change over time. Physicians focus on clinical care, not billing mechanics. Documentation that feels adequate clinically may still fall short for billing. Requirements for medical necessity, critical care, procedures, and medical decision-making are nuanced, and many gaps only surface when denials arrive weeks later.
How to Identify If Your ED Is Making These Errors
Before fixing documentation errors, you need to know whether they are happening and which types are driving the most impact.
Review Denial Patterns
Pull denial data for the past six months. What percentage cite “insufficient documentation” or “medical necessity not established”? If more than 5 percent are documentation-related, you likely have a systemic issue. Look for patterns in which error types appear most frequently, and track whether the rate is increasing over time.
Audit Sample Charts
Pull 20 random charts from the past month. Score each against the five error types, then calculate the percentage with each error. If 15 percent have weak medical necessity documentation, you can extrapolate annual exposure. For example, 15 percent of 50,000 visits at a $75 average loss equals $562,500 in annual risk from that error alone.
Analyze HIM Query Volume
How many queries does HIM send physicians each week, and what do they typically ask for? The query pattern usually mirrors your most common documentation gaps. High query volume signals a recurring problem. Each query represents a chart that could not be billed as submitted, delaying reimbursement.
Check These Red Flags
A high percentage of level 4 visits compared to level 5 can indicate that charts are not consistently supporting higher complexity. Emergency departments often bill 30 to 40 percent of visits at level 5. If you are substantially below that range, it can suggest insufficient MDM documentation.
Low procedure billing relative to volume may mean procedures are being performed but not documented completely. Minimal critical care billing despite high-acuity patients can indicate that time is not being captured. Frequent payer medical record requests can signal that payers are questioning documentation quality.
Simple Assessment Questions
Do physicians document in real time or finish charts hours later? Retrospective documentation increases error risk.
How often do completed charts get returned for clarification?
What is your denial rate for documentation reasons? A reasonable target is under 3 percent.
How many hours per week do physicians spend responding to queries about their charts?
How AI Prevents Each Error Type
Artificial intelligence trained on emergency medicine billing requirements can identify documentation gaps in real time and prompt clinicians to fill missing elements before the chart is signed. The goal is prevention at the point of care, not discovery weeks later in denials, downcoding, or audit activity.
Medical Necessity Documentation
AI can recognize when a chart does not clearly justify why emergency department evaluation was required. It reviews what is already documented and flags when medical necessity is not explicitly established.
Real-time prompts guide physicians to capture key elements such as symptom severity, acuity, risk factors, and why ED-level resources were warranted.
Example: A patient presents with chest pain. The physician documents the basics but does not include cardiac risk factors or high-risk characteristics. AI prompts: “Consider documenting cardiac risk factors and symptom characteristics to support medical necessity for ED evaluation.” The physician adds two sentences that reduce denial risk.
Procedure Documentation
AI can detect when a procedure is referenced but not documented with the elements required for billing. It flags incomplete procedures before chart closure.
Prompts help ensure documentation includes indication, technique, findings, complications, and time when applicable. This reduces the common failure mode where the procedure is performed and discussed but not fully captured in the chart.
Example: A note mentions “laceration repaired” but there is no procedure documentation. AI flags it before signing: “Laceration repair mentioned but no procedure note found. Please complete procedure documentation.” The physician completes it quickly. Revenue protected: $150 to $250.
Critical Care Time
AI can recognize when the presentation and documented interventions align with critical care criteria, then prompt for time and supporting justification.
It helps ensure documentation includes total time and a clear rationale showing the patient met critical care thresholds and required sustained physician attention.
Example: A septic patient requires continuous monitoring and multiple interventions. The physician documents the course but does not include time. AI prompts: “This case may meet critical care criteria. Please document start and stop times and total minutes.” The physician confirms 55 minutes. Revenue protected: $300 to $400.
Medical Decision-Making Completeness
AI can assess whether the documented MDM supports the billed complexity level. It checks for differential diagnosis breadth, data reviewed and interpreted, patient risk, and decision-making complexity.
Feedback helps clinicians see when a chart may be clinically accurate but still thin on the reasoning auditors and payers expect.
Example: A complex multi-system presentation is documented with diagnosis and treatment but limited reasoning. AI feedback: “Current documentation supports level 4. To support level 5, consider documenting differential diagnosis and interpretation of studies.” The physician adds a few sentences. Downcode risk decreases. Revenue protected: $60.
Billing-Critical Elements
AI can run completeness checks before chart sign-off. It verifies that core documentation components are present and that key orders have clear indication documented.
Catching gaps at the point of care reduces HIM queries, shortens billing cycle time, and lowers the chance that claims get held or delayed.
Example: A physician is ready to sign. AI flags: “Cardiovascular exam findings not documented” and “CT abdomen ordered without documented indication.” The physician adds the missing elements in under a minute. Query avoided and the claim can move forward.
The Financial Result
In the Elite Hospital Partners case study, emergency medicine physicians using DocAssistant were associated with $399,168 in additional annualized revenue per physician. This was not upcoding or billing for services not delivered. It reflected better capture of care already being provided, supported by stronger medical necessity documentation, more complete procedure capture, more consistent critical care time documentation, clearer MDM support for appropriate billing levels, and fewer incomplete charts at submission.
These systems work best when prompts are specific and contextual, tied to emergency medicine documentation and billing standards, and delivered at the moment the gap can be fixed quickly.
Building the Business Case for Error Prevention
Once you confirm your emergency department is experiencing these errors, the case for prevention is usually clear.
For Finance Leadership
Start by estimating your current exposure using the assessment framework. Audit a sample of charts for each error type, calculate the percentage affected, then multiply by annual visit volume and the estimated cost per error.
Example: “Our audit shows 12 percent of charts have medical necessity gaps. At 50,000 annual visits and a $75 average loss, we are losing $450,000 annually from this error alone. Across all five error types, total exposure is approximately $1.2 million.”
Then compare that exposure to the cost of prevention. AI-based documentation support typically costs $100,000 to $200,000 annually for a mid-size emergency department. If it prevents 40 percent of errors, that recaptures roughly $480,000 in previously lost revenue. In many departments, that supports a 6 to 12 month payback, with ongoing benefit afterward. Use your own volume and error rates to calculate a department-specific ROI.
For Clinical Leadership
Position prevention as physician support, not criticism. These errors are rarely about competence. They are a predictable outcome of trying to produce billing-compliant documentation under intense time pressure while managing multiple sick patients.
A tool that prevents errors in real time reduces burden. Fewer queries on patients seen days ago. Less post-shift clean-up. Less uncertainty about whether documentation is complete. Real-time guidance helps physicians capture the right details while the encounter is still fresh.
For Compliance and Risk Leadership
Error prevention is risk mitigation. Stronger documentation improves audit defensibility. Fewer denials can reduce payer scrutiny. More consistent documentation quality across providers lowers compliance exposure. Frame the investment as compliance protection, with revenue preservation as an additional return.
Implementation Approach
Start with a structured pilot focused on measurable outcomes. Test AI-based error prevention with a subset of physicians and track documentation-related denial rates, query volume, time to bill, and revenue per encounter. Compare pilot results to baseline or a control group, then expand based on measured reductions in errors and documented financial impact.
Conclusion
Documentation errors in emergency departments can cost hospitals $500,000 to $2 million annually, but many of the most common issues are preventable. These gaps are typically driven by workflow pressure, time constraints, and multi-patient management, not physician shortcomings.
The five most expensive error types are incomplete medical necessity documentation, missed procedure documentation, undocumented critical care time, insufficient medical decision-making to support the billed level, and missing billing-critical elements. Each has a measurable financial impact and often represents revenue leakage for care already delivered.
Technology trained on emergency medicine billing requirements can catch documentation gaps in real time and prompt clinicians for missing elements before chart closure. That helps prevent errors instead of discovering them weeks later after revenue is lost. Done well, this approach protects revenue, reduces retrospective queries, improves audit defensibility, and supports appropriate reimbursement for complex emergency care.
To determine where your department is most exposed, audit a sample of recent charts to identify which error patterns occur most often. You can also request a documentation assessment to quantify your exposure or review case studies showing measured impact from emergency departments using error prevention technology.
About the Author
Nathan Murray, M.D. Emergency Medicine - Founder of DocAssistant
Dr. Nathan Murray is an Emergency Medicine trained physician and the founder of DocAssistant. With years of frontline clinical experience, Dr. Murray is passionate about using AI to streamline medical documentation and enhance clinical decision making.
