Before and After implementation. Quantifying AI revenue impact in the ED.
AI scribe ROI claims are everywhere. Real before and after implementation data is harder to find. This article breaks down what actually changes when a purpose-built ED platform goes live - and why the architecture behind the tool determines whether the revenue follows.
The ROI claims around AI scribes have proliferated faster than the evidence behind them. Every vendor has a case study, every pitch deck has a percentage, and by now most revenue cycle directors and ED administrators have heard versions of the same story enough times that the specifics have stopped landing.
This article takes a different approach. Rather than presenting a single outcome in isolation, it compares what the research and real-world implementations consistently show across departments before and after AI scribe adoption - looking at billing accuracy, revenue capture, documentation completeness, and denial rates - and explains precisely which design variables determine whether an ED sees those outcomes or doesn't.
The difference between departments that recover significant revenue and departments that see minimal financial return from AI scribing isn't luck. It's architecture.
The Revenue Problem That Exists Before Any Tool Is Introduced
Before any before/after comparison is meaningful, it helps to be precise about what the baseline problem actually is. Emergency departments are not losing revenue because they're billing incorrectly. They're losing revenue because their documentation isn't capturing the full complexity of the care they're delivering.
Since January 2023, ED evaluation and management coding has been determined entirely by Medical Decision Making complexity. Every element of MDM - the number and complexity of problems addressed, the amount and complexity of data reviewed and analyzed, and the risk of complications - must be explicitly documented in the note for the billing level to be supported. Care that was delivered but not documented to the required level of specificity bills at a lower level than the clinical complexity justifies.
This isn't a compliance problem. It's a documentation architecture problem. Physicians making high-complexity decisions under time pressure, documenting from memory after the encounter, systematically leave out MDM elements - not because they didn't address them clinically, but because reconstructing the full reasoning in a note an hour later is cognitively demanding under the conditions that define an emergency shift.
The revenue gap this creates is not marginal. It is the gap between what an ED bills and what it could defensibly bill if documentation captured clinical complexity in real time, accurately and completely. Every AI scribe claim about revenue recovery is, at its core, a claim about closing that gap. The question is how much of it gets closed, and why.
What the Broader Research Shows - Real Comparisons Across Departments
The research on AI scribe revenue impact has matured significantly over the past two years, and the findings across different health systems and care settings are now specific enough to be genuinely useful for comparison.
A January 2026 study from the University of California San Francisco published in JAMA Network Open found that physicians with access to ambient AI scribes generated 5.8% more weekly relative value units - a key productivity metric tied to revenue generation - and saw 2.8% more patients per week. Claims weren't denied more often despite the higher coding activity, which is a meaningful finding given the audit concerns some organizations carry about AI-assisted documentation. That RVU increase translates, using 2025 Medicare rates, to roughly $3,000 more revenue per physician per year at the aggregate level - a modest but statistically validated number.
A larger implementation at The Permanente Medical Group, tracked over 63 weeks across more than 2.5 million patient encounters and published in NEJM Catalyst, found that AI scribes saved an estimated 15,791 hours of documentation time across 7,260 physicians. Departments with historically high documentation burdens - including emergency medicine - saw the highest adoption rates and the most pronounced efficiency gains.
A Trilliant Health analysis of national all-payer claims data across six large health systems that had publicly adopted AI scribes found consistent upward redistribution of evaluation and management visits toward higher-complexity billing codes. Riverside Health in Virginia saw an 11% rise in physician work relative value units and a 14% increase in documented Hierarchical Condition Category diagnoses per encounter. Northwestern Medicine clinicians using ambient AI scribes billed more high-level E/M visits on average.
These numbers are meaningful. They're also, in the context of emergency medicine under 2023 MDM guidelines, conservative relative to what purpose-built ED platforms deliver. The UCSF study and the Permanente data reflect general clinical environments and general-purpose ambient tools. Emergency medicine, where billing complexity is highest and MDM documentation requirements are most specific, is where the delta between a general-purpose tool and a purpose-built one shows up most clearly.
Before and After - What the Comparison Actually Looks Like
The most useful way to present this data is as a direct before/after comparison across the metrics that matter most to an ED revenue cycle team. The following composite represents what the research and real-world implementations consistently show across emergency departments that have adopted purpose-built AI scribing with integrated MDM billing analysis.
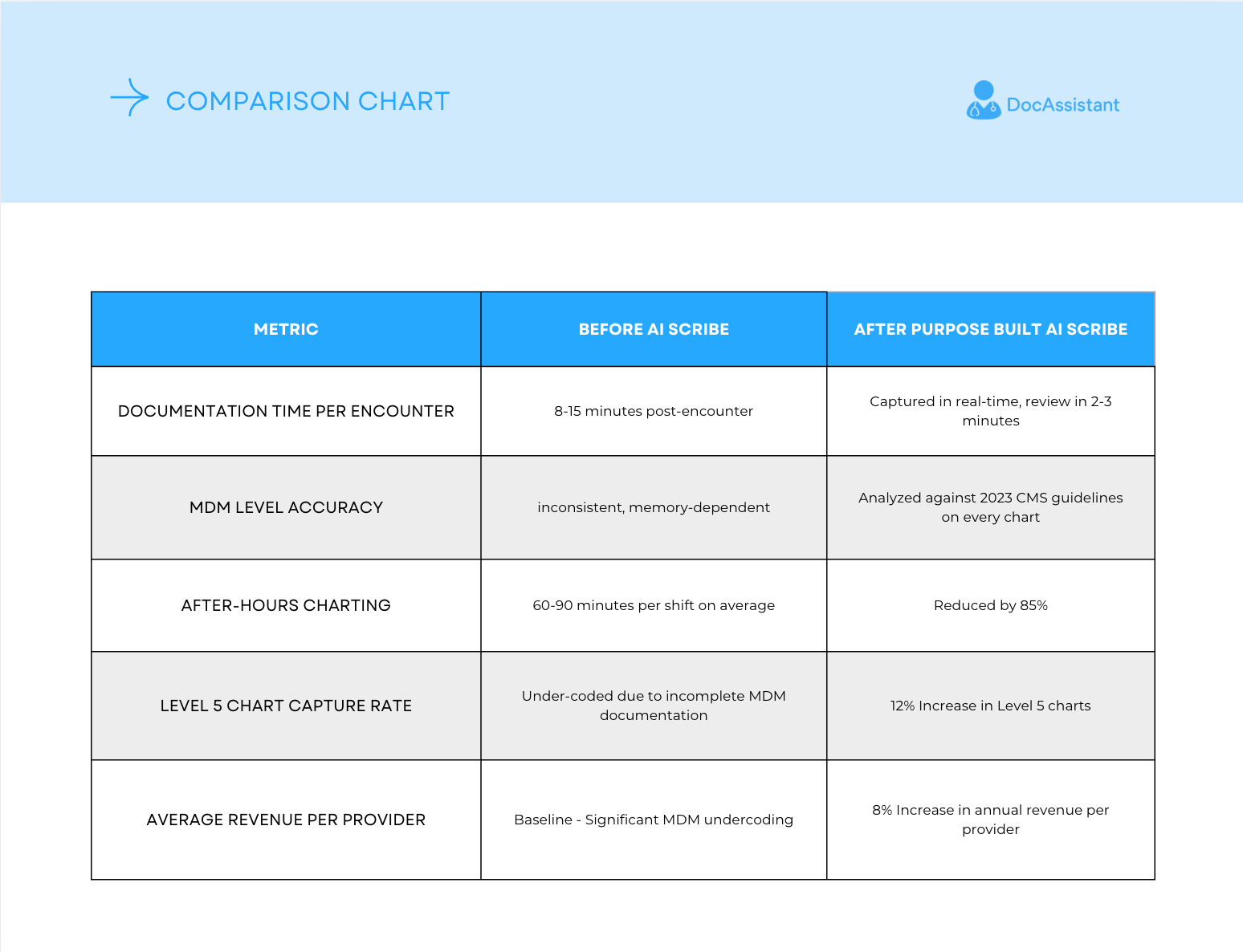
Those last two rows deserve more than a table cell. A 12% increase in Level 5 chart capture sounds like a documentation metric - but in emergency medicine billing, it's a revenue event. Level 5 is the highest E/M billing level in an ED encounter, reserved for cases involving high-complexity MDM: multiple diagnoses, extensive data review, and high risk of morbidity or mortality. When a physician manages a high-complexity patient and the note doesn't capture the MDM elements that support Level 5 coding, the chart bills at Level 4 or lower - not because the care wasn't high-complexity, but because the documentation didn't reflect it.
At current Medicare rates, the reimbursement gap between a Level 4 and Level 5 ED E/M code is approximately $80-$120 per encounter. In a department seeing 40,000 patients annually, moving even 5% of those encounters from Level 4 to the Level 5 they clinically supported represents $160,000 to $240,000 in recovered revenue - before accounting for commercial payer differentials, which are typically higher. An 8% increase in average revenue per provider compounds further across a multi-provider department. These aren't inflated projections. They're the direct financial translation of documentation completeness - capturing what was clinically done and letting the billing reflect it accurately.
What Partners Say About the Shift
Numbers tell one part of the story. The physicians and administrators who have lived the before/after transition tell another - and in emergency medicine, where physician adoption is the variable that determines whether any tool actually delivers its potential, that perspective matters.
"Our groups were struggling with note compliance and timeliness until I found DocAssistant. Since we implemented it across all of our sites, we've had fantastic note compliance and a 12% bump in our Level 5 charts, plus all our docs absolutely love the time saving and cognitive offload. Hands down the best AI Scribe for the Emergency Department."
Dr. David Darrigan, DO, FAACP - President, Elite Hospital Partners
"We met Nathan and his team at ACEP, and their solution stood out immediately among all scribe vendors. After piloting the platform, our medical director said after just one shift that we had to keep it. Within a month, improved reimbursement and workflow efficiencies made expansion an easy decision. Outstanding team, seamless onboarding, and measurable impact - this is the best technology we've implemented."
Dr. Elizabeth James, MD, FACEP - CEO, Keystone Medical Group
Two things stand out across both accounts that the research data alone doesn't capture. First, the speed of the signal - one shift for a medical director to recognize the impact, one month for expansion to become an easy decision. Second, the dual nature of what's being described: note compliance and billing improvement happening simultaneously, not as separate initiatives but as the same outcome. That's what documentation completeness looks like in practice. When notes are complete, compliant, and captured in real time, the billing follows naturally - no separate coding effort required.
The Revenue Risk Question - Addressing It Honestly
Any honest discussion of AI scribe revenue optimization has to address the legitimate concern about audit exposure. As AI scribing has driven coding intensity upward across health systems, payers have responded. Starting in October 2025, Cigna began automatically reducing many level 4–5 E/M claims by one level unless documentation clearly supports higher complexity. Aetna Better Health has applied similar reviews. A PMC policy brief examining this dynamic concluded that while near-term revenue gains are real, late adopters may miss the temporary upside while still practicing under a lower baseline rate set after everyone else's gains have been priced in.
This is a real risk, and the organizations best positioned to navigate it are the ones whose revenue gains are driven by documentation completeness rather than coding optimization. There is a meaningful difference between a tool that helps a physician document the full complexity of the care they actually delivered and a tool that coaches them to code at higher levels regardless of clinical complexity. The former is defensible under any payer scrutiny because the documentation supports the claim. The latter isn't.
The compliance safety principle here is straightforward: MDM-driven revenue recovery is defensible when the documentation accurately reflects clinical reality. The 12% increase in Level 5 charts documented through DocAssistant is not a product of upcoding - it's a product of physicians finally having a documentation tool that captures the MDM complexity they were already managing but not fully recording. When Cigna or Aetna reviews those charts, the documentation supports the billing level. That's the difference between revenue recovery that holds up and revenue recovery that creates exposure.
Four Variables That Determine Whether an ED Sees the Revenue Outcome
The before/after comparison looks compelling in aggregate. Whether any specific ED sees those outcomes depends on four variables that most vendor comparisons don't make explicit.
1. Whether MDM billing analysis is built into the documentation workflow or absent entirely.
This is the single most important variable. A tool that transcribes accurately but doesn't analyze whether the documented content supports the appropriate MDM level is solving a time problem, not a revenue problem. The revenue gap in emergency medicine exists specifically at the MDM analysis layer - and a tool without that layer leaves the gap intact. Every comparison showing modest RVU improvements from general-purpose ambient tools versus the outcomes from purpose-built ED platforms reflects this architectural difference more than any other factor. The 12% Level 5 improvement and 8% average revenue increase at Elite Hospital Partners didn't come from transcription speed. They came from real-time MDM analysis on every chart.
2. Whether the tool is EHR-agnostic or bundled.
Bundled EHR tools deliver AI scribing as a feature of a larger platform contract. The billing analysis depth in bundled tools is typically shallow because it wasn't the core product - it was an add-on feature. EHR-agnostic platforms built specifically for ED billing optimization deliver the analytical depth that recovery at scale requires.
3. Whether adoption is genuine or nominal.
The research on AI scribe ROI consistently shows a dose-response relationship - physicians who use the tool for more than 40% of their encounters see dramatically better outcomes than low-intensity users. Revenue recovery doesn't happen at low adoption rates, regardless of how well the platform performs technically. The Keystone Medical Group experience - expansion decided within a month of pilot - reflects what high-intensity adoption looks like when the tool is genuinely embedded in the clinical workflow from day one.
4. Whether the revenue reporting is transparent and ongoing.
Revenue recovery claims made at the point of sale are theoretical. The organizations seeing sustained financial improvement are the ones with ongoing reporting that tracks MDM level distribution, undercoding patterns, and revenue capture per provider over time. If a vendor can't show you that reporting in a live demo, the revenue claim is retrospective marketing rather than operational infrastructure.
The DocAssistant AI Outcome - What the Case Data Shows
With those four variables as the evaluation framework, the Elite Hospital Partners implementation provides the most relevant before/after comparison for emergency departments actively evaluating purpose-built AI scribing.
Across providers in that implementation:
- 12% increase in Level 5 chart capture
- 8% increase in average revenue per provider
- $399,000 recovered per provider per year in previously lost revenue
Those numbers came from a real ED environment - not a controlled pilot with hand-selected encounters - running the platform across standard patient volume and standard shift conditions.
The recovery mechanism was the MDM billing analyzer - reviewing every chart against 2023 CMS E/M guidelines in real time, flagging undercoding before submission, and prompting physician review at the attestation step. The clinical care didn't change. The documentation captured it more completely, and the billing reflected that completeness. The Level 5 chart increase is the visible expression of that mechanism: encounters that were already high-complexity but previously documented at lower levels, now captured accurately.
Mapped against the four evaluation variables: MDM billing analysis is integrated into the core workflow, not an add-on. The platform is EHR-agnostic. Implementation includes physician onboarding designed to drive high-intensity adoption from day one. Revenue reporting is built into the platform and tracks outcomes over time. For anyone still weighing what drives that difference at a technical level, the documentation and billing optimization design is worth reviewing in detail.
The Internal Case - What to Bring to a Revenue Cycle or CFO Conversation
For anyone in the organization who has worked through this data and now needs to make the case to leadership, the argument distills to this:
The revenue gap that AI scribing closes is not theoretical. It exists in every ED where physicians are documenting from memory rather than capturing clinical complexity in real time. The 2023 MDM coding change made that gap explicitly visible - every chart either supports the billing level or it doesn't, and the documentation is the only thing that determines which.
The financial math for a ten-provider emergency department at the Elite Hospital Partners outcome level is approximately $3.9 million in annual revenue recovery. Not from seeing more patients, not from changing clinical practice, and not from billing at levels the care doesn't support - from ensuring that the care already being delivered is documented completely enough to be billed at the level it actually justifies. The 8% increase in average revenue and the 12% increase in Level 5 chart capture are the mechanisms that produce that number, encounter by encounter, shift by shift.
The risk of not addressing this isn't neutral. Every shift that runs without MDM billing analysis is a shift where that gap persists. It compounds monthly, quarterly, annually, in ways that are entirely recoverable once the right documentation infrastructure is in place - and entirely invisible until it is. For revenue cycle teams trying to understand what the cost structure looks like against that return, the pricing model comparison across AI scribe vendors is worth working through before making a final decision.
What to Do Next
The before/after data in this article establishes a clear picture: purpose-built ED AI scribing with integrated MDM billing analysis produces revenue outcomes that general-purpose ambient tools don't, and the architectural differences that explain the gap are specific and evaluable before signing any contract.
The organizations seeing the most significant financial return from AI scribe adoption are the ones that evaluated those variables carefully - not the ones that moved fastest or chose the most visible vendor. For emergency departments and health systems that want to see how that evaluation maps to their specific volume, EHR environment, and current MDM coding patterns, DocAssistant AI offers a structured assessment session designed for revenue cycle teams and clinical leadership. The analysis of what your department is currently leaving on the table is available before any commitment is made. For compliance and governance teams who also need to understand the audit defensibility of AI-generated documentation alongside the revenue picture, the governance framework that makes this approach defensible is worth reviewing alongside this analysis.
About DocAssistant
DocAssistant is an AI-powered medical scribe, clinical decision support platform, and point-of-care billing tool built for acute care. Founded by practicing emergency physicians and headquartered in San Diego, California, DocAssistant reduces documentation time by over 80%, optimizes billing in real time against 2023 CMS E&M guidelines, and delivers evidence-based clinical recommendations backed by 9,000+ peer-reviewed articles. HIPAA-compliant and trusted by emergency and acute care physicians across the United States.
docassistant.ai | hello@docassistant.ai | (619)-344-0849
Nathan Murray
DocAssistant
+1 619-344-0849
Visit us on social media: