
What Data Shows About Burnout, Documentation Time, and Patient Outcomes
Physicians spend nearly half their clinical time on documentation rather than patients. The data connecting that burden to burnout, diagnostic quality, and revenue loss is more specific — and more actionable — than most organizations have fully reckoned with.
An emergency physician finishes a ten-hour shift. The department has quieted. The last patient has been seen. But the physician isn't leaving. They're sitting at a workstation with fourteen charts still open, knowing that the next two hours belong not to rest or family or recovery — but to documentation. Care that was delivered hours ago, now being reconstructed from memory at the end of a shift that should have ended at 7pm.
This isn't an anecdote. It's a pattern — and the data behind it is more consequential than most healthcare organizations have fully reckoned with.
The Numbers Behind the Burden
The scale of the documentation problem in American medicine is not a matter of debate. The numbers are well established, consistently replicated, and still somehow underweighted in most organizational conversations about physician performance and patient care quality.
The AMA's most recent data on physician time allocation shows that in 2024, physicians reported a 57.8-hour average workweek — with only 27.2 of those hours spent on direct patient care. Another 13 hours went to indirect patient care including documentation, order entry, and results review. And 22.5% of physicians reported spending more than eight hours outside normal working hours on the EHR each week. Those aren't hours spent improving care. They're hours spent reconstructing it on paper after the fact.
In emergency medicine, the picture is even sharper. Research from Yale published in JAMA Network Open found that ED physicians spent nearly four times as much time on documentation as on EHR review — a ratio that raises serious questions about whether the documentation model currently in place is structured for the environment it's supposed to serve. Emergency medicine is a specialty built on rapid assessment, pattern recognition, and high-stakes decision-making under time pressure. The documentation burden it currently carries is structurally at odds with all three.
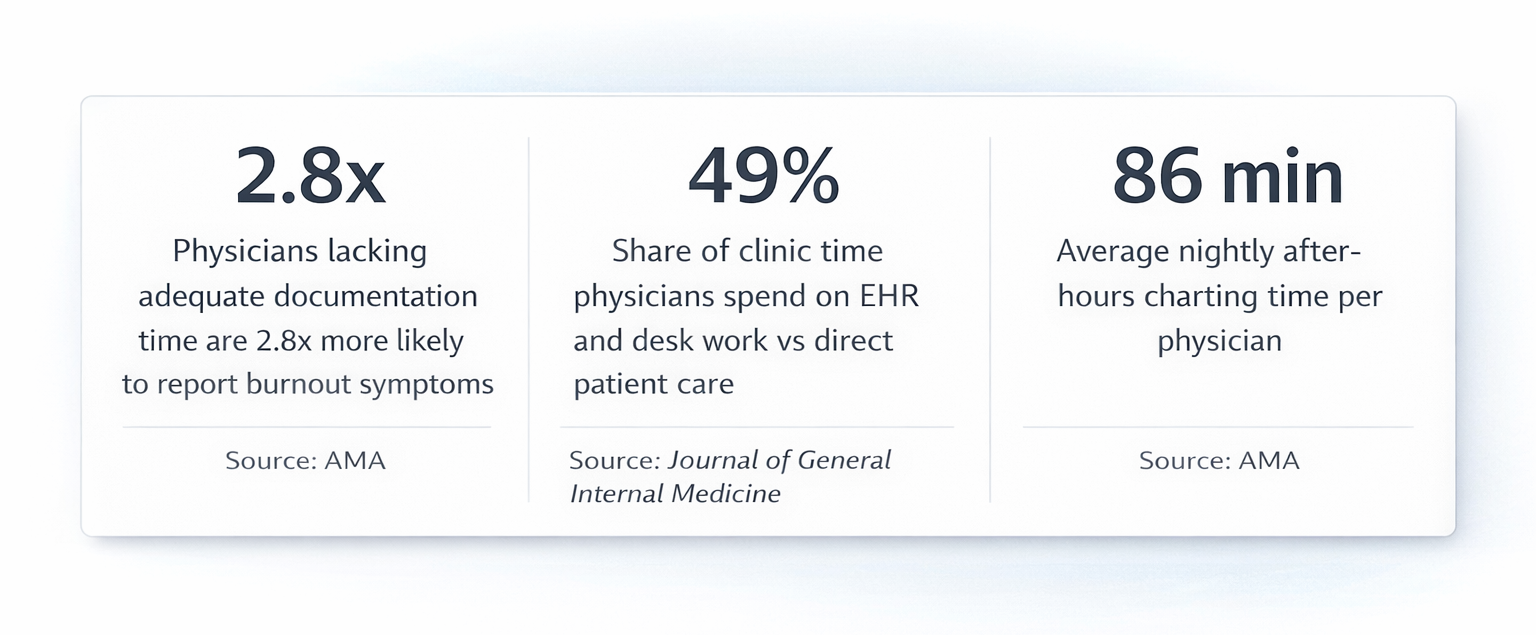
The number that anchors everything else: physicians spend 49% of their clinic time on EHR and desk work versus direct patient interaction. Not a majority of their time with patients. A majority of their time on administrative tasks that exist around patients.
What Happens to Patients When Physicians Are Burned Out
Burnout tends to get discussed as a physician welfare issue — which it is. But framing it exclusively that way obscures its most consequential dimension: what happens to patients when the physician caring for them is cognitively depleted, running behind on documentation, and operating in a state of chronic administrative overload.
The research on this is consistent and sobering across three specific mechanisms.
Diagnostic accuracy
Cognitive fatigue impairs the quality of clinical decision-making. A physician finishing charts at midnight is not operating at the same diagnostic capacity as one who documented in real time during the encounter and ended their shift with cognitive reserves intact. The specific risk in emergency medicine — where diagnostic errors carry immediate clinical consequences — is that documentation-driven fatigue is invisible. It doesn't show up in any metric until something goes wrong.
Handoff quality
Incomplete or delayed documentation directly degrades handoff quality at shift transitions. When notes aren't finished before a shift change, the incoming provider is working from verbal memory-based handoffs rather than documented clinical reasoning. In a fast-moving ED where a patient's status can change significantly in two hours, that gap is not theoretical.
Patient interaction
When documentation burden consumes a larger share of each encounter, the time and cognitive presence available for the patient decreases. Research consistently shows that patients detect this — burnout correlates with lower patient satisfaction scores, reduced perceived empathy, and decreased trust in the care relationship. The physician who is mentally managing fourteen open charts while seeing the next patient is not fully present for either task.
The Revenue Consequence Nobody Talks About
Burnout is a physician wellness problem. It's a patient safety problem. It's also a revenue problem — and this is the dimension that gets the least airtime in organizational conversations, despite being the most directly quantifiable.
The financial cost of documentation burden operates through three distinct mechanisms, each of which compounds the others.
Undercoding from fatigue
When physicians are finishing charts from memory hours after the encounter, the clinical complexity of what happened in that room gets systematically undersold. MDM elements that were genuinely part of the encounter — external records reviewed, risk stratification tools applied, clinical reasoning about what was considered and ruled out — get omitted. Not because the care wasn't delivered. Because the physician documenting at 11pm doesn't remember every element of the encounter they managed at 2pm, and the documentation model gives them no mechanism to capture it in real time. Every omitted element is a billing level that doesn't get supported. Multiplied across every encounter in a shift, across every shift in a year, the revenue impact is substantial. The financial mechanics of documentation-driven revenue loss in emergency medicine run deeper than most revenue cycle teams have quantified.
Claim denials from incomplete documentation
Nearly one in five medical claims is initially denied, and 60% of those denials are never resubmitted. Incomplete documentation is a primary driver. A physician running behind on charts and documenting from fatigue is more likely to produce notes that fail payer scrutiny — not because the care was inadequate, but because the documentation doesn't reflect its full complexity. The clinical reality and the documented record diverge, and the divergence costs money.
Physician turnover cost
Burned-out physicians leave. The cost of replacing a physician in emergency medicine — recruiting, credentialing, privileging, onboarding, and productivity ramp — runs between $500,000 and $1 million per departure. Documentation burden is consistently cited among the top drivers of physician attrition. That means the documentation problem isn't just a revenue leakage issue — it's also quietly funding one of the most expensive line items in ED operations.
The Documentation Time–Outcome Curve
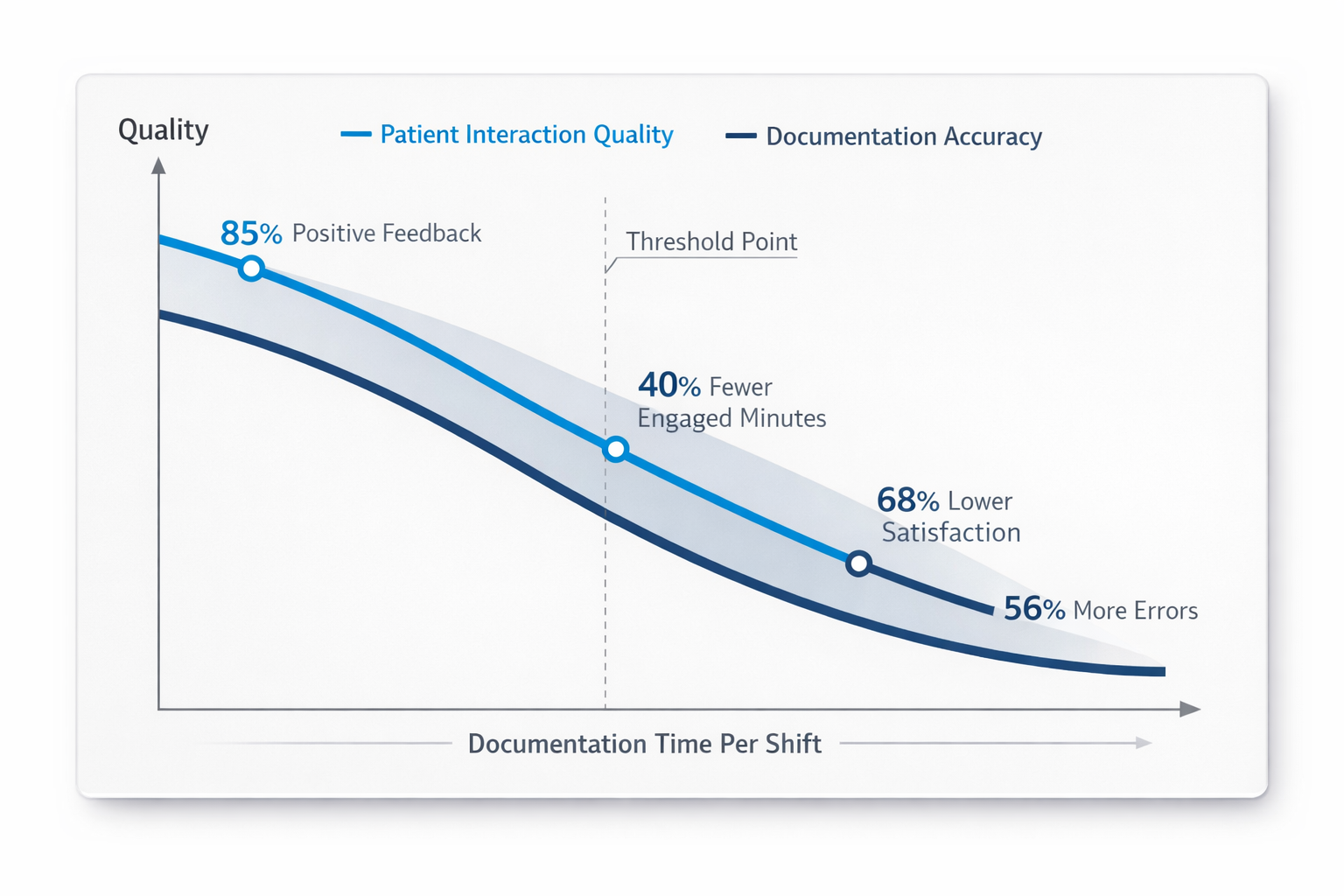
Documentation time and patient care time aren't independent variables. They exist on a curve within a fixed shift, where one increases at the direct expense of the other. This isn't a new observation — it's been implicit in every conversation about physician burnout for the past decade. What's changed is how specifically the data now quantifies it.
As documentation time increases beyond a threshold, direct patient interaction time decreases. Cognitive load increases. And both diagnostic accuracy and documentation completeness suffer simultaneously — because the same cognitive resources that drive good clinical decisions also drive good clinical documentation. A physician who is mentally exhausted from three hours of post-shift charting doesn't return the next day with full reserves. The depletion carries forward.
The implication of this curve is structural, not individual. The physicians experiencing it aren't undisciplined or inefficient. They're operating in a documentation model that structurally produces this tradeoff — one that asks them to deliver care and document care as two separate sequential activities, when the evidence suggests that separating them is exactly what degrades the quality of both.
Changing the outcome requires changing the model, not the physician.
What the Research Says Works
Before getting to any specific platform or product, it's worth being precise about what the evidence actually supports — because not all documentation interventions produce the same results, and the research on this is now specific enough to be useful.
Three categories of intervention have meaningful evidence behind them.
1. Team-based documentation support
Research published in JAMA Internal Medicine found that physicians who adopted team-based documentation support at high intensity — meaning more than 40% of note text contributed by another team member — saw significant reductions in EHR time including after-hours charting, along with increases in visit volume. The critical finding was in what didn't work: low-intensity adoption produced almost no measurable benefit. The intervention only delivered results when it was genuinely embedded in the workflow, not technically available but rarely used. This finding applies to every category of documentation support that follows.
2. Structured specialty-specific note templates
Departments that implement ED-specific note templates reduce documentation time and improve coding accuracy by reducing the cognitive load of note construction from scratch. The benefit is most pronounced in high-volume environments where the number of distinct encounter types is large and time per encounter is constrained. Templates alone don't solve the problem — but they're a meaningful component of any documentation redesign.
3. AI-assisted ambient documentation
This is the most recent and most significant category. Multiple studies now show that ambient AI documentation tools, when purpose-built for the clinical environment and adopted at sufficient intensity, reduce documentation time by 50–85%, reduce after-hours charting substantially, and improve note completeness and billing accuracy. The adoption intensity finding from team-based documentation applies here too — the benefit is proportional to how deeply the tool is integrated into clinical workflow, not simply whether it's installed.
The through-line across all three categories: the intervention has to change the documentation model, not just add a tool to an unchanged workflow. Physicians who continue to document the same way they always have, with an AI tool nominally available but not integrated, see outcomes similar to those of low-intensity adopters in the team-based documentation research. Almost none.
What This Looks Like in Emergency Medicine Specifically
Emergency medicine sits at the intersection of every variable this article has covered. It has the highest documentation volume per shift, the most complex MDM billing requirements under the 2023 CMS E&M guidelines, the most cognitively demanding clinical environment, and among the highest burnout rates of any specialty. It's also the environment where the documentation-outcome connection is most direct — because every ED encounter carries an immediate billing consequence tied to the clinical complexity documented in the note.
The interventions described above have been tested and validated in this environment. What that looks like in practice — in a real ED, with real volume, under real operational conditions — is documented in the Elite Hospital Partners implementation of DocAssistant AI. Physicians in that implementation reduced charting time by 85% and recovered an average of $399,000 per provider per year in previously lost revenue. Not by changing how they practiced medicine. By changing how their documentation was captured, structured, and analyzed against 2023 CMS MDM requirements in real time.

That outcome closes the loop on everything the data in this article describes. The physician who isn't finishing charts at midnight is more cognitively available for the next shift. The note that captures MDM complexity in real time is more complete and more billing-accurate than one reconstructed from memory at the end of a shift. The department that addresses documentation burden at the model level reduces burnout, improves diagnostic availability, improves note quality, and recovers revenue — simultaneously, through the same intervention. For anyone still weighing what that translates to in practice, the numbers behind that outcome are worth reviewing in full.
The Organizational Equation
When documentation burden gets discussed as a wellness issue, organizations respond with wellness programs. When it's framed as a clinical quality issue, they respond with quality improvement initiatives. When it's discussed as a revenue issue, they respond with revenue cycle tools.
What the data in this article shows is that it's all three simultaneously — and that addressing it at the documentation layer addresses all three at once. For any ED administrator or CMO trying to build the internal case for a documentation intervention, the organizational math is straightforward.
For a ten-provider emergency department:
Documentation time recovered:
85% reduction per provider, eliminating most after-hours charting and recovering cognitive bandwidth for clinical care
Revenue recovered:
At $399,000 per provider per year, a ten-provider ED is looking at approximately $3.9 million in annual revenue recovery from documentation that was already being delivered but not captured at the right billing level
Turnover risk reduced:
Fewer burned-out physicians means lower attrition and lower replacement cost — meaningful in a specialty where each departure costs between $500,000 and $1 million
Audit defensibility improved:
More complete, consistent, real-time documentation reduces denial rates and reduces OIG exposure from incomplete or undercoded charts
For anyone working through how to evaluate the cost structure of AI documentation tools against that return, the pricing and ROI framework is worth understanding before making a vendor decision.
The case for acting on this data isn't complicated. What's complicated is continuing to absorb the cost of not acting — in physician burnout, in revenue leakage, in diagnostic availability, and in the turnover cycles that quietly drain emergency departments of their most experienced providers.
The Bottom Line
Back to that physician at the workstation. Fourteen charts open. Shift ended two hours ago.
The data in this article doesn't change what that moment feels like. But it does change how an organization should interpret it — not as one physician's endurance problem, but as a structural documentation design failure with a measurable clinical, operational, and financial cost. A cost that is being paid every shift, in every ED still running on a model that separates documentation from care delivery and asks physicians to absorb the difference.
The organizations addressing this most effectively aren't asking their physicians to document faster or more efficiently within the existing model. They're changing the model — removing the documentation burden from the physician's cognitive load and capturing it in a way that is more accurate, more complete, and more billing-appropriate than the current approach produces.
If your department is ready to see what that looks like in practice, DocAssistant AI offers a pilot built around your specific ED volume, EHR environment, and documentation workflow. The data behind that conversation is already in this article.
About DocAssistant
DocAssistant is an AI-powered medical scribe, clinical decision support platform, and point-of-care billing tool built for acute care. Founded by practicing emergency physicians and headquartered in San Diego, California, DocAssistant reduces documentation time by over 80%, optimizes billing in real time against 2023 CMS E&M guidelines, and delivers evidence-based clinical recommendations backed by 9,000+ peer-reviewed articles. HIPAA-compliant and trusted by emergency and acute care physicians across the United States.
docassistant.ai | hello@docassistant.ai | (619)-344-0849
Nathan Murray
DocAssistant
+1 619-344-0849
Visit us on social media:

