
The True ROI of AI Scribes in High-Volume Emergency Departments
High-volume emergency departments see $399K additional revenue per physician annually with AI scribes. Real case data shows 85% charting time cuts and measurable ROI.

Most emergency departments think of AI scribes as a 'charting time saver.' But that misses the bigger picture: AI scribes are revenue recovery tools that prevent hospitals from losing money they've already earned. AI scribes aren't productivity tools that happen to generate revenue. They're revenue recovery systems that happen to save time.
The difference matters because it changes how you evaluate the return on investment. When viewed as a time-saving tool, AI scribes compete with other efficiency measures. When viewed as revenue recovery, they're compared against money currently being lost - and the business case becomes obvious.
This article quantifies the true ROI (return on investment) of AI scribes in high-volume emergency departments using real implementation data, peer-reviewed research, and system-level financial modeling. The numbers are specific. The mechanisms are measurable. And the timeline to positive return is shorter than most administrators expect.
The Revenue Problem AI Solves
Emergency departments don't have a "charting is slow" problem. They have a "we can't bill for work we're already doing" problem.
High-volume ED's lose revenue in three measurable ways. Firstly, physicians miss billable procedures because documentation competes with critical patient care. A physician managing a septic patient doesn't formally document the shoulder reduction performed between resuscitation tasks. The reduction happened. The patient benefited. But without proper documentation, it's unbillable.
The second is when complex medical decision-making gets downcoded because charts don't capture physician thought process. An emergency physician evaluating undifferentiated chest pain considers cardiac ischemia, pulmonary embolism, aortic dissection, pneumothorax, and esophageal rupture. They order troponin, d-dimer, chest imaging, and ECG. The differential diagnosis drives complex risk stratification. But if the chart documents only "chest pain, studies negative, discharged," payers see a simple case and reimburse accordingly. The complexity happened. The risk management was real. But the revenue doesn't match the work.
Lastly, the final way High-volume ED's lose revenue is when critical care time goes undocumented and physicians can't track start and stop times during active resuscitation. A physician spends 60 minutes managing DKA (diabetic ketoacidosis)-continuous monitoring, multiple interventions, frequent reassessment. But documentation happens later when details are fuzzy. Without clear time documentation and critical care criteria articulation, the case bills as a level 5 visit instead of critical care. Revenue lost: $300 to $400 per case.
Unfortunately, these aren't just theoretical problems. Research demonstrates that insufficient medical decision-making documentation is a primary driver of downcoding in emergency medicine, where clinical complexity consistently exceeds what appears in charts.
A study between Elite Hospital Partners and DocAssistant quantified this revenue leakage directly. Before AI scribe implementation, their emergency physicians were experiencing typical documentation-related revenue loss. After implementation, physicians recovered $399,168 in additional annual revenue per provider. This wasn't from seeing more patients or up-coded charts. It was from billing appropriately for work already being performed.
What AI Scribe ROI Actually Looks Like in High-Volume ED's
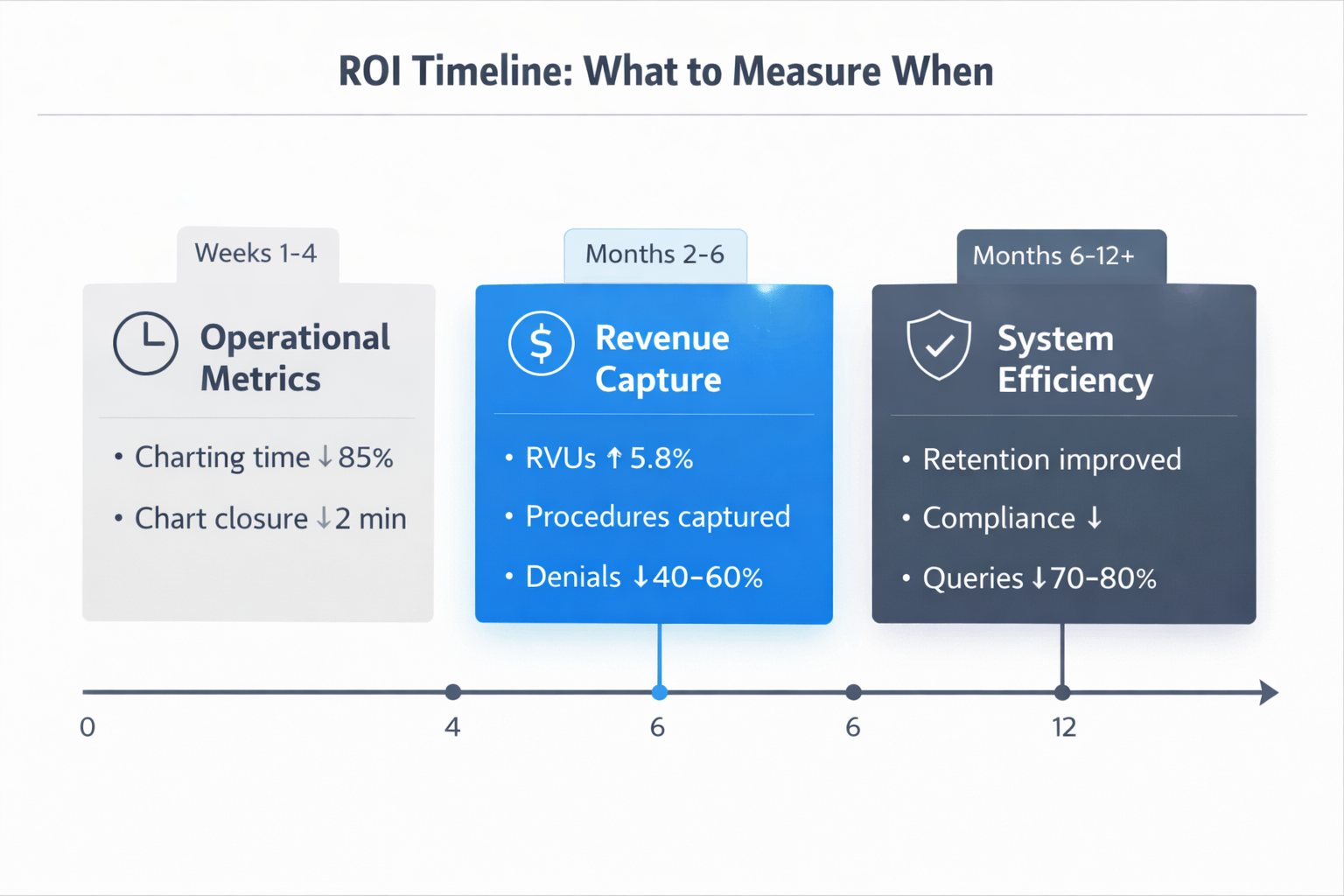
ROI for AI scribes & Co-Pilots has three distinct phases: immediate operational improvement, near-term revenue capture, and long-term system efficiency gains.
Immediate Phase (Weeks 1-4): Operational Metrics
Charting time drops within days of implementation. The Elite Hospital Partners study showed 85% reduction in documentation burden. Physicians who previously spent 90-120 minutes per shift on charts now spend 15-20 minutes reviewing AI-generated documentation.
This time doesn't just disappear - it redistributes to patient care. Emergency physicians spend nearly 44% of their shift on documentation compared to only 28% with patients. AI scribes reverse that ratio. More time at bedside means faster clinical decision-making, improved patient throughput, and reduced waiting room times.
Chart closure accelerates dramatically. Human scribes typically complete charts 1-3 hours after patient encounters. AI scribes close charts within 2 minutes of patient departure. When charts close faster, billing happens sooner, and cash flow improves.
Near-Term Phase (Months 2-6): Revenue Capture
Revenue improvements appear in monthly billing data within 60-90 days. The mechanisms are specific and measurable.
Procedure capture improves immediately. AI-based systems recognize when procedures are mentioned but not formally documented. Real-time prompts ensure physicians complete procedure notes before chart closure. A recent study found that physicians using AI scribes generated 5.8% more weekly relative value units, seeing 2.8% more patients per week without increased denial rates.
Medical necessity documentation strengthens across all charts. AI systems trained on emergency medicine billing requirements identify when charts lack sufficient justification for ED-level evaluation. Denial rates for medical necessity drop measurably.
Critical care billing increases when appropriate. AI recognizes patient presentations and documented interventions meeting critical care criteria. Prompts help physicians document time and complexity.
AI makes sure doctors' notes clearly show how complex the case was. This ensures the hospital gets paid the right amount for the level of care provided. Real-time feedback prevents downcoding by ensuring charts capture differential diagnosis, data interpretation, and risk assessment.
The Elite Hospital Partners case study showed these improvements translated directly to revenue: $399,168 additional annual revenue per physician. For a 12-physician emergency department, that's $4.79 million in annual revenue recovery. For a 20-physician department, it's $7.98 million annually.
Long-Term Phase (Months 6-12+): System Efficiency
Sustained implementation produces compounding benefits that exceed initial projections.
Physician retention improves measurably. When charting time drops 85%, job satisfaction increases. Physician replacement costs exceed $200,000 per provider when accounting for recruiting, onboarding, and productivity ramp time. Preventing even one departure per year justifies significant AI investment.
Compliance exposure decreases over time. Stronger documentation quality means better audit defensibility. Payer scrutiny decreases when documentation consistently supports billed levels.
Query volume drops dramatically. When AI ensures completeness before closure, query burden essentially disappears. This saves Health Information Management (HIM) labor costs and accelerates revenue cycle by eliminating clarification delays.
Research on AI-assisted clinical documentation confirms that these findings demonstrate measurable improvements in coding accuracy and completeness, with direct impact on revenue capture across emergency department settings.
The Business Case: Calculating Your Department's Specific ROI
Most AI scribe ROI calculations focus on cost per physician. That approach misses how return scales with volume, acuity, and current revenue leakage.
Step 1: Calculate Current Revenue Loss
Start with baseline assessment. Pull six months of denial data and identify documentation-related denials. What percentage cite insufficient medical necessity, incomplete MDM(medical decision making), or missing elements? Calculate average loss per denial.
Review procedure billing against visit volume. If your ED sees significant trauma, orthopedic injuries, and lacerations but procedure billing seems low relative to volume, documentation gaps likely exist. Audit sample charts to estimate undocumented procedure frequency.
Assess critical care billing patterns. High-volume ED's should bill critical care regularly given acuity. If critical care represents less than 3-5% of high-acuity visits, time documentation gaps probably exist.
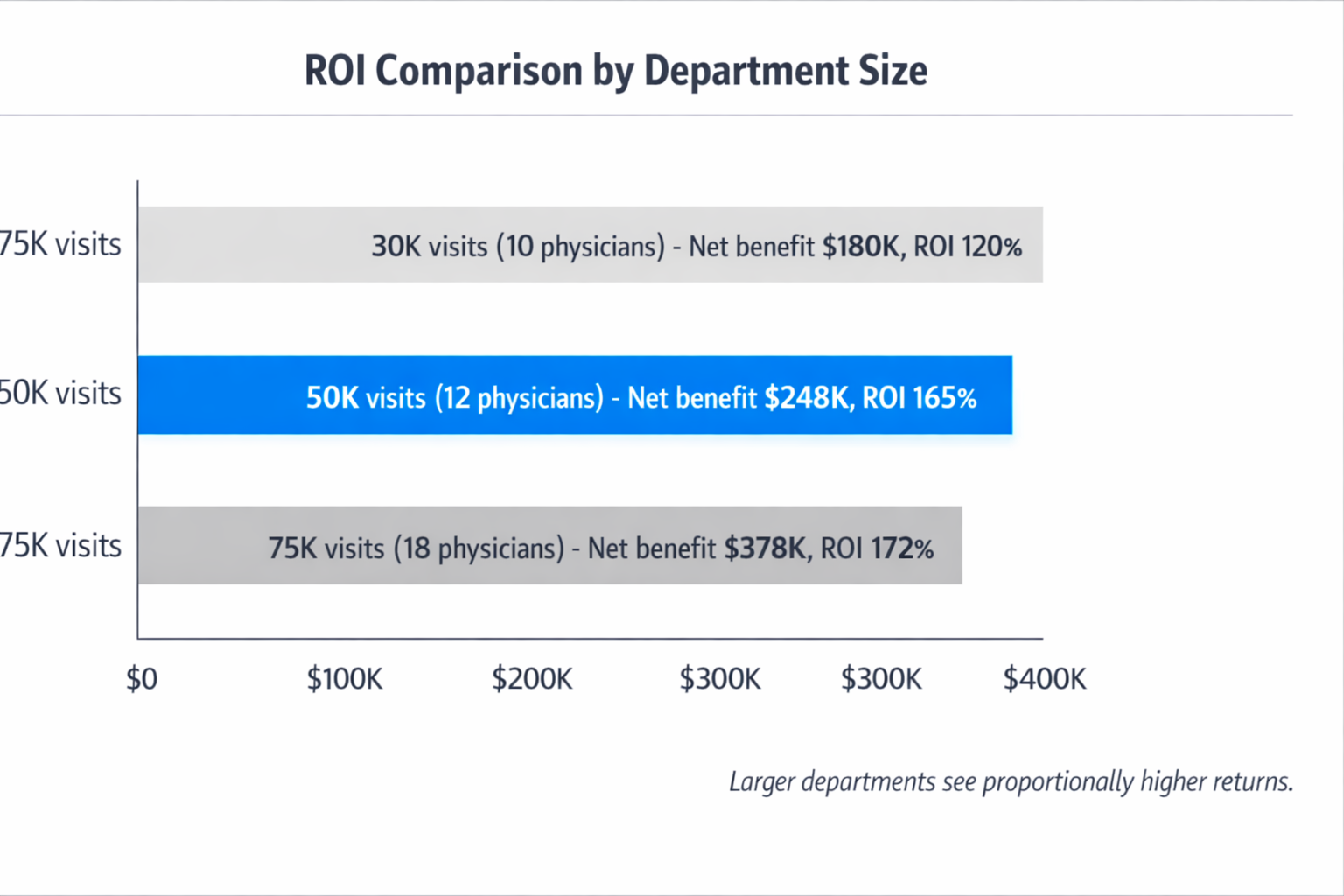
Example calculation for a 50,000-visit ED with 12 physicians:
- Documentation-related denials: 5% of visits at $75 average loss = $187,500 annually
- Undocumented procedures: 5 per physician monthly at $200 average = $144,000 annually
- Missed critical care: 2 cases per physician monthly at $350 loss = $100,800 annually
- Downcoding from insufficient MDM: 15% of level 4-5 visits at $60 loss = $180,000 annually
Total current revenue leakage: $612,300 annually
Step 2: Project Revenue Recovery
AI scribes don't eliminate 100% of documentation-related revenue loss, but they address the majority. Conservative modeling assumes 60-70% capture of currently lost revenue.
Using the example above:
- Current leakage: $612,300
- Recovery rate: 65%
- Projected revenue capture: $398,000 annually
This aligns closely with the Elite Hospital Partners finding of $399,168 per physician in a similar-volume environment.
Step 3: Calculate Net ROI
AI scribe costs for mid-size emergency departments typically range from $100,000 to $200,000 annually depending on physician count and visit volume. Using $150,000 as mid-range cost:
- Revenue recovery: $398,000
- AI scribe cost: $150,000
- Net benefit: $248,000 annually
- ROI: 165%
- Payback period: 5.5 months
This calculation excludes additional benefits like physician retention (worth $200,000+ per prevented departure), reduced HIM labor for queries, and compliance risk reduction.
Step 4: Account for Volume and Acuity Scaling
ROI improves with volume and acuity. Higher-volume departments see proportionally greater return because larger departments lose more money from documentation gaps, but AI scribe costs don't increase at the same rate
Higher-acuity departments benefit more from procedure and critical care capture. Level 1 trauma centers (hospitals that treat the most severe injuries) with significant procedural volume see larger revenue recovery than lower-acuity community EDs.
Example: A 75,000-visit Level 1 trauma center with 18 physicians might see:
- Current revenue leakage: $920,000 annually
- AI scribe cost: $220,000 annually
- Projected recovery (65%): $598,000
- Net benefit: $378,000 annually
- ROI: 172%
Implementation Realities: What Actually Affects ROI
ROI projections only work when implementation accounts for emergency department workflow realities.
Physician Adoption Timeline
ROI calculations assume physicians actually use the system. Training time for AI scribes averages 11 minutes per physician. This minimal learning curve enables rapid deployment without disrupting operations.
Physician buy-in accelerates when early users report results. Starting with 2-3 physician champions who document their experience creates momentum. When colleagues see 85% charting time reduction and faster chart closure, adoption spreads organically.
The Elite Hospital Partners implementation demonstrated this pattern. Physicians who used the system for 60+ days showed the full $399K revenue impact.
Integration with Existing Workflows
AI scribes succeed when they fit existing physician documentation patterns rather than forcing workflow changes. Systems that require structured templates or specific documentation sequences create friction.
EHR (Electronic Health Record) integration determines whether AI scribes accelerate or complicate workflows. Direct EHR integration where AI documentation flows automatically into appropriate fields eliminates manual copy-paste friction.
Mobile accessibility matters in high-volume emergency departments where physicians move constantly. AI scribes accessible via smartphone or tablet enable documentation from anywhere.
Measuring ROI in Practice
Most departments track the wrong metrics when evaluating AI scribe success. Charting time reduction is interesting but doesn't directly tie to financial return. Revenue-focused metrics show true impact.
Track these specific indicators monthly:
- RVUs per physician per shift (should increase 5-8% within 90 days)
- Procedure billing volume (should increase 20-30% if significant gaps existed)
- Critical care billing frequency (should increase if appropriate cases were previously underbilled)
- Documentation-related denial rate (should decrease 40-60%)
- HIM query volume (should decrease 70-80%)
- Average days to bill submission (should decrease 30-40%)
The Elite Hospital Partners case study tracked exactly these metrics and documented measurable improvement across all categories.
Real-World Implementation Results: Beyond the Elite Case Study
While the Elite Hospital Partners case study provides the most detailed documentation of AI scribe ROI in emergency medicine, other health systems report similar findings.
Kaiser Permanente achieved 65-70% physician adoption of AI scribe technology across their system, indicating the value proposition works at scale. Their emergency physicians saved 15,791 hours of documentation time in one year—equivalent to eight full-time physicians focusing entirely on patient care instead of paperwork.
A physician-level analysis across multiple health systems found that providers using AI scribes for 60 days or more saw approximately one hour per day reduction in documentation time. This time savings translated to 5.8% more RVUs generated weekly and 2.8% more patients seen per week.
BJC Health System and Washington University School of Medicine reported that 65% of providers using their AI scribe solution for 60+ days saw documentation time reduction of about an hour daily. This consistent finding across multiple organizations validates the operational benefits seen in the Elite study.
Emergency-specific implementations show even stronger results. Departments implementing AI scribe technology report 15-20% improvements in patient throughput as documentation delays disappear. When physicians can close charts in under two minutes rather than hours later, patient flow accelerates measurably.
Comparing AI Scribes to Human Scribes
Human scribes have proven value. A systematic review and meta-analysis published in Annals of Emergency Medicine found that scribes improved RVUs per hour, patients per hour, and provider satisfaction.
However, human scribe programs face structural challenges. Staffing shortages, training time (typically 3-6 months), turnover, and scheduling complexity create operational burden. Cost per physician for human scribes typically ranges from $40,000 to $60,000 annually when accounting for wages, benefits, training, and turnover.
AI scribes provide comparable documentation quality without staffing challenges. They cost less per physician ($25,000 to $35,000 typically), work 24/7 without breaks or sick days, require minimal training, and deliver consistent quality regardless of shift timing or patient volume.
For high-volume EDs, the scalability advantage of AI scribes produces better ROI. A 20-physician department would need 40-60 human scribes to provide coverage across all shifts—that's $1.6-$3.6 million in annual scribe cost plus operational overhead. The same department would pay $500,000-$700,000 for AI scribes covering all physicians 24/7.
Building the Internal Business Case
Securing approval for AI scribe investment requires translating ROI analysis into language that resonates with different stakeholders.
For Finance Leadership
Frame AI scribes as revenue recovery, not expense. The current state includes $400,000-$900,000 in annual revenue leakage. AI scribes cost $150,000-$250,000 annually and capture 60-70% of lost revenue.
Present conservative projections with documented assumptions. Use your own denial data, procedure billing patterns, and critical care frequency to build department-specific models. Even if revenue recovery is only 50% of projections, ROI remains strongly positive.
Quantify physician retention value. Preventing one departure saves $200,000+ in recruiting and onboarding costs. If AI scribes improve physician satisfaction enough to reduce turnover by even one physician every other year, that's $100,000+ annual value.
For Clinical Leadership
Position AI scribes as physician support, not surveillance. Emergency physicians need tools that eliminate administrative burden so they can focus on clinical care.
Highlight work-life balance impact. When physicians stop staying late to finish charts, job satisfaction improves. The 85% charting time reduction means physicians can actually leave when their shift ends.
Address quality concerns proactively. Better documentation means better communication with consultants and admitting teams. Stronger medical decision-making documentation protects physicians in the event of litigation by clearly showing clinical reasoning.
For Hospital Administration
Connect AI scribes to strategic priorities. Most hospitals have identified physician burnout, revenue cycle improvement, and operational efficiency as key objectives. AI scribes directly address all three.
Show competitive positioning. As more health systems implement AI scribes, departments without them face recruiting disadvantages. Emergency physicians increasingly expect AI documentation support.
Frame as risk mitigation. Stronger documentation reduces compliance exposure. Better medical necessity justification means fewer audits. The compliance value exists independent of revenue impact.
Implementation Roadmap for High-Volume EDs
Successful AI scribe implementations follow a structured approach that minimizes disruption while accelerating time to value.
Phase 1: Assessment and Planning
Quantify current state using the framework outlined earlier. Pull denial data, assess procedure billing, evaluate critical care frequency. Build your department-specific revenue leakage model.
Identify physician champions. Find 2-3 physicians who are both well-respected by peers and genuinely interested in reducing documentation burden.
Establish baseline metrics. Document current charting time, RVUs per physician, procedure billing volume, critical care frequency, denial rates, and HIM query volume.
Phase 2: Pilot Implementation
Start with champion physicians. Get them using the system consistently and documenting their experience. Track their charting time, revenue metrics, and satisfaction weekly.
Within 4-6 weeks, champion physicians should show measurable charting time reduction and improved chart completion rates. By 8-12 weeks, revenue metrics should start improving if documentation gaps are being addressed.
Share results transparently. Show all physicians what champions are experiencing. Concrete data from trusted colleagues drives adoption better than vendor marketing materials.
Phase 3: Department-Wide Rollout
Expand to all interested physicians. Focus on getting 60-70% adoption within the first six months. Provide implementation support immediately available during shifts when physicians encounter questions.
Continue measuring consistently. Track the same metrics established at baseline. Share results monthly with all stakeholders.
Phase 4: Optimization and Scale
By month 12, target 90%+ of physicians using AI scribes routinely. Validate ROI with real data comparing month 12 metrics to baseline.
Document and share success. Build your own case study showing before-and-after results. This supports future technology investments and validates the AI scribe decision to stakeholders.
When AI Scribes Don't Make Sense
AI scribes aren't the right solution for every emergency department. Understanding when the business case doesn't work prevents poor investments.
Very low-volume departments (under 15,000 visits annually) may not have enough revenue leakage to justify AI scribe costs. If absolute revenue loss is only $100,000-$150,000 annually, and AI scribes cost $100,000+, the margin is too thin.
Departments with very simple case mix where most visits are truly low-acuity may not experience significant documentation-related revenue loss. If undercoding isn't happening because cases genuinely are simple, AI scribes won't recover much revenue.
EDs where physicians already use comprehensive templates effectively and denial rates are very low (under 2%) have less to gain. If documentation is already strong, the marginal improvement from AI scribes may not justify the cost.
Departments unwilling to measure results objectively shouldn't implement AI scribes. Without baseline metrics and ongoing measurement, you can't validate ROI or optimize the system.
Conclusion
The ROI of AI scribes in high-volume emergency departments isn't theoretical—it's measurable, substantial, and achievable within 6-12 months.
The Elite Hospital Partners case study demonstrated $399,168 in additional annual revenue per physician with 85% reduction in documentation burden. Multiple health systems report similar results: measurable revenue increases, significant time savings, and improved physician satisfaction.
The business case comes down to simple math. High-volume emergency departments lose $400,000-$900,000 annually to documentation-related revenue leakage. AI scribes cost $150,000-$250,000 annually. They capture 60-70% of lost revenue while simultaneously reducing physician administrative burden and improving job satisfaction.
For most high-volume EDs, the question isn't whether AI scribes generate positive ROI. The question is how quickly you can implement them to stop losing money you're already earning but failing to capture.
The path forward is straightforward: quantify your current revenue leakage, pilot with physician champions, measure results rigorously, and scale based on demonstrated impact. The departments implementing AI scribes today are recovering revenue their competitors are still losing.
If your emergency department sees 40,000+ visits annually, has documentation-related denial rates above 3%, or loses billable procedures and critical care time to incomplete documentation, the business case for AI scribes already exists. The only question is when you'll act on it.
About the Author
Nathan Murray, M.D. Emergency Medicine - Founder of DocAssistant
Dr. Nathan Murray is an Emergency Medicine trained physician and the founder of DocAssistant. With years of frontline clinical experience, Dr. Murray is passionate about using AI to streamline medical documentation and enhance clinical decision making.


